Are you confused about recommendations for breast cancer screening mammograms?
Do you have questions like these?
- When should I begin?
- How often do I need to be screened?
- What are the associated risks?
If so, join the club! You’re not alone!
Plenty of people have questions about mammogram screening recommendations, and for good reason. Even the experts don’t agree.
Here are the current recommendations for women who are under an average risk for breast cancer:
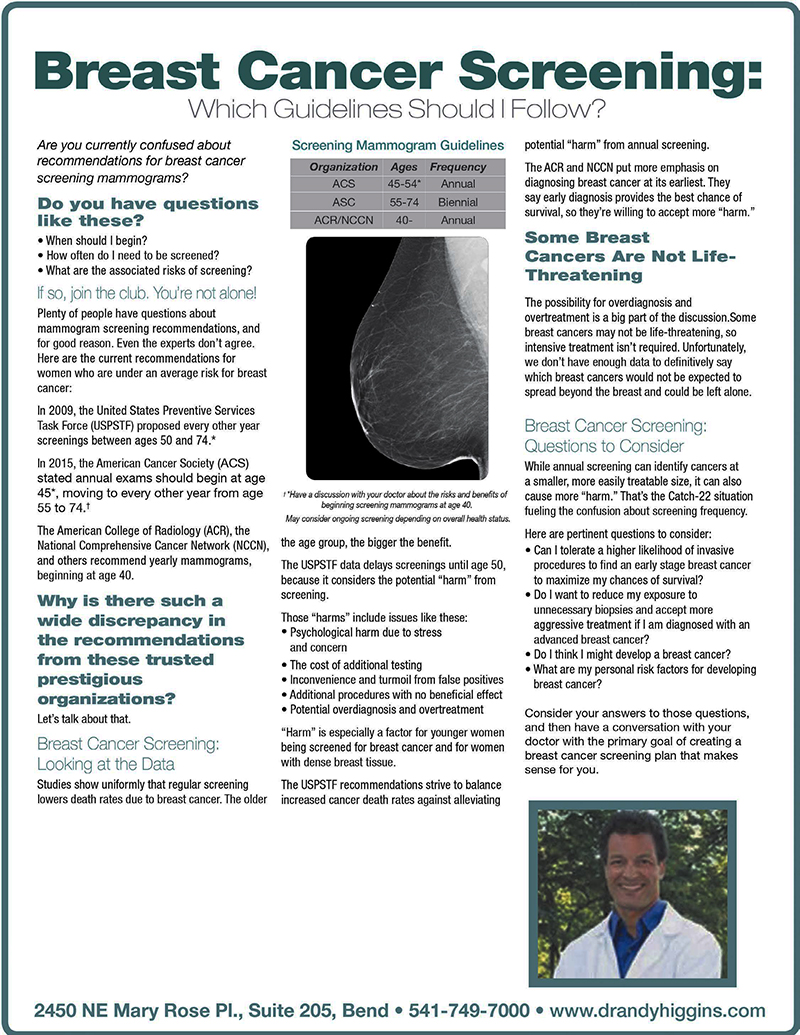
- The 2009 United States Preventive Services Task Force (USPSTF) proposed every other year screenings, beginning at age 50.
- The American Cancer Society (ACS) says annual exams should begin at age 45, moving to every other year at age 55.
- The American College of Radiology (ACR), National Comprehensive Cancer Network (NCCN) and others recommend yearly mammograms, beginning at age 40.
Why is there such a wide discrepancy in the recommendations from these trusted prestigious organizations?
Let’s talk about that.
Breast Cancer Screening: Looking at the Data
Studies show uniformly that regular screening lowers death rates due to breast cancer. The older the age group, the bigger the benefit.
The USPSTF data delays screenings until age 50, because it considers the potential “harm” from screening.
Those harms include issues like these:
- Psychological harm due to stress and concern
- The cost of unnecessary testing
- Inconvenience and turmoil from false positives
- Unnecessary procedures with no beneficial effect
- Harm from radiation exposure
Harm is especially a factor for younger women low risk factors for breast cancer and for women with dense breast tissue.
The USPSTF recommendations strive to balance increased cancer death rates against alleviating potential harm from annual screenings.
The ACR and NCCN put more emphasis on diagnosing breast cancer at its earliest. They say early diagnosis provides the best chance of survival, so they’re willing to accept more “harm.”
Some Breast Cancers are Not Life-Threatening
The possibility for over-diagnosis and over-treatment is a big part of the discussion.
Some breast cancers may not be life threatening, so intensive treatment isn’t required.
Unfortunately, we don’t have enough data to definitively say which breast cancers would not be expected to spread beyond a contained local site (remain in situ) and could be left alone.
Breast Cancer Screening: Questions to Consider
While annual screening can identify cancers at a smaller size, it can also cause more harm. That’s the Catch-22 situation fueling the confusion about screening frequency.
Here are pertinent questions to consider:
- Is it more important for me to maximize my chances for survival or lower the risk of harm?
- Will I accept standard treatment recommendations (if diagnosed with breast cancer), or would I look for alternative treatments?
- When should I start and stop screening?
- What are my personal risk factors for developing breast cancer?
Consider your answers to those questions, then have a conversation with your primary care physician with the primary goal of creating a breast cancer screening plan that makes sense for you.
Please Note: The articles on Dr. Andy Higgins’ website are obtained from a variety of sources. While they pertain to the treatment of breast cancer, colon cancer, and other maladies, their presence here is not to help diagnose or treat any disease, but to stimulate conversation about health-related issues. All articles are cleared by an editor, but not necessarily by Doctor Higgins himself.